
The information in this brief is intended for educational use only.
This brief provides a summary of the CHOICES Learning Collaborative Partnership simulation model of a $0.02-per-ounce state excise tax on sugar-sweetened beverages (SSB). The tax, which would be administered by the Washington State Department of Revenue (DOR), aims to reduce consumption of calorie-dense, nutrient-poor beverages.
The Issue
Although SSB consumption has declined in recent years, children and adults in the United States consume twice as many calories from SSBs compared to 30 years ago.1 – 3 Research has linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. SSB consumption may increase the risk of developing chronic diseases via effects on body mass index (BMI) and other mechanisms.4-5 The Dietary Guidelines for Americans, 2015,6 recommends reduced SSB intake to help manage body weight. Drawing upon the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on unhealthy foods and beverages.7-10 In 2009, the Institute of Medicine recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an appropriate target for taxation.11
About the SSB Tax
In this model, the state excise tax would apply to bottlers and distributors and be passed on directly to consumers in full as part of the price of the product. The tax would apply to all beverages with added caloric sweeteners but not to 100 percent juices, milk products, or artificially sweetened beverages. The $0.02-per-ounce excise tax would increase SSB prices in the state of Washington by 24.4 percent. Implementation would require the state DOR to communicate the tax to bottlers and process tax statements; it would require businesses to prepare tax statements for state audits using private tax accountants.
Comparing Costs and Outcomes
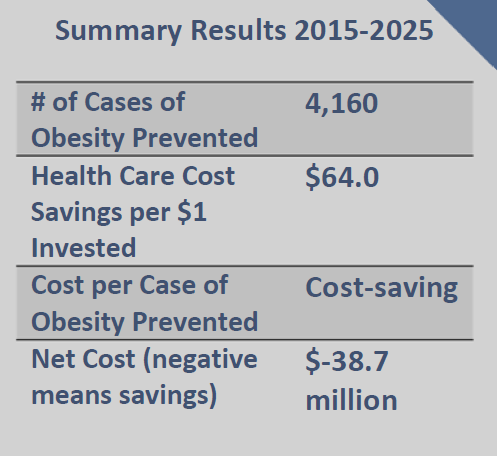
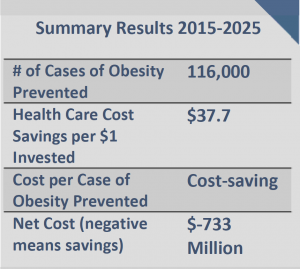
CHOICES cost-effectiveness analysis compared the costs and outcomes of the SSB excise tax over 10 years with costs and outcomes associated with not implementing the tax.
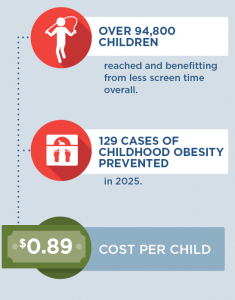
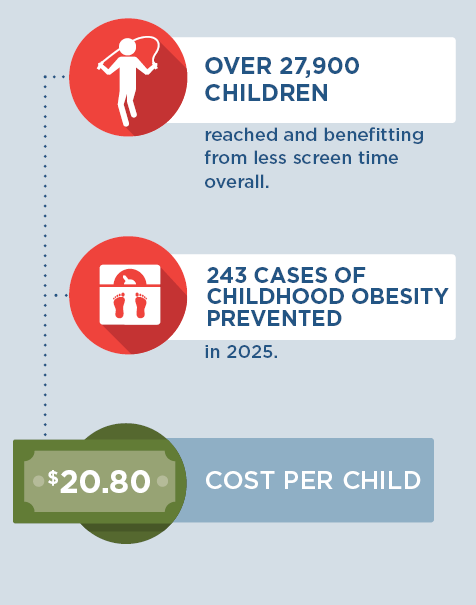
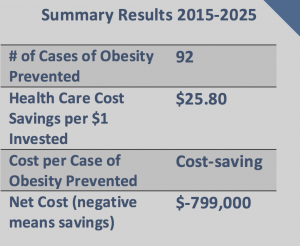
Implementing a state $0.02-per-ounce sweetened beverage tax in Washington is an investment in the future. By the end of 2025: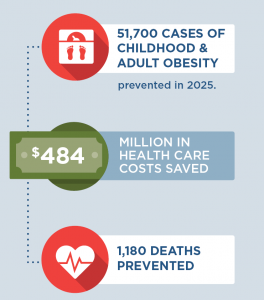 |
Conclusions and Implications
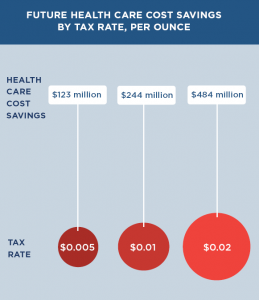
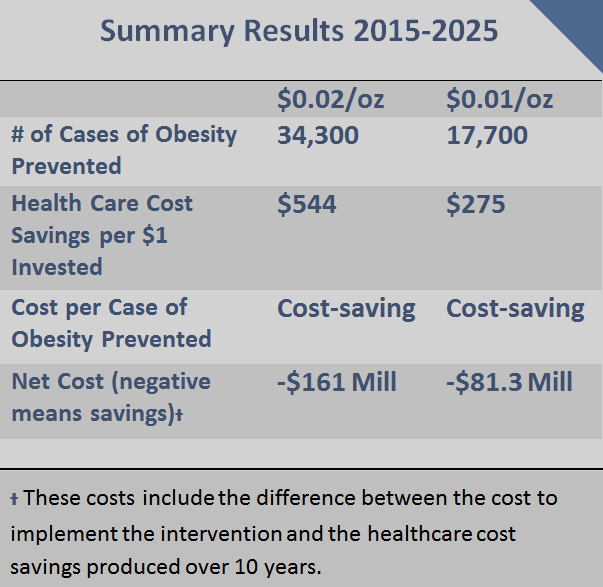
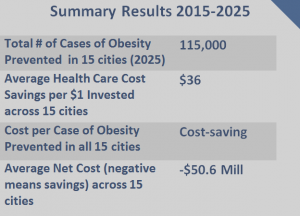
According to this model analysis, a $0.02-per-ounce sweetened beverage tax on SSBs in Washington would reach all residents of the state and prevent 8,380 cases of childhood obesity and 43,300 cases of adult obesity in 2025. The tax would also prevent deaths while reducing future health care costs. Lower tax rates such as $0.01 or $0.005 per ounce would have less of an impact on health and health care cost savings.
In other locations that have looked at this issue, there are concerns about the impact of the tax on low-income households. This analysis indicates that households will spend less on SSBs after the tax takes effect, therefore increasing income for other purchases. In addition, greater health benefits will accrue to low-income consumers, who on average consume more SSBs than higher-income consumers. The same is true for certain racial and ethnic groups. Thus, disparities in obesity outcomes should decline following implementation of the proposed tax. In addition, revenue from the SSB tax could be reinvested in low-income communities.
 |
References
- Wang YC, Bleich SN, and Gortmaker SL. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988–2004. Pediatrics. 2008;121(6):e1604-e1614.
- Nielsen SJ and Popkin BM. Changes in beverage intake between 1977 and 2001. Am J Prev Med. 2004; 27(3):205-210.
- Bleich, SN, Wang YC, Wang Y, Gortmaker, SL. Increasing consumption of sugar-sweetened beverages among US adults: 1988–1994 to 1999—2004. Am J Clin Nutr. 2008; 26883
- Malik VS, Pan A, Willett WC, Hu FB. Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am J Clin Nutr. 2013;98(4):1084-1102.
- Chen L, Caballero B, Mitchel DC, Loria C, et al. Reducing consumption of sugar-sweetened beverages is associated with reduced blood pressure a prospective study among United States adults. Circulation. 2010;121(22):2398-2406
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015 – 2020 Dietary Guidelines for Americans. 8th Edition. December 2015. Available at http://health.gov/dietaryguidelines/2015/guidelines/.
- Chaloupka FJ, Powell LM, Chriqui JF. Sugar-sweetened beverage taxes and public health: A Research Brief. Minneapolis, MN: Robert Wood Johnson Foundation, Healthy Eating Research, 2009.
- Brownell KD, Farley T, Willett WV, et al. The public health and economic benefits of taxing sugar-sweetened beverages. New Engl J Med. 2009;361(16):1599-1605.
- Long MW, Gortmaker SL, Ward ZJ, Resch SC, Moodie ML, Sacks G, Swinburn BA, Carter RC, Claire Wang Y. Cost Effectiveness of a Sugar-Sweetened Beverage Excise Tax in the U.S. Am J Prev Med. 2015 Jul;49(1):112-23.
- Gortmaker SL, Wang YC, Long MW, Giles CM, Ward ZJ, Barrett JL, Kenney EL, Sonneville KR, Afzal AS, Resch SC, Cradock AL. Three Interventions That Reduce Childhood Obesity Are Projected To Save More Than They Cost To Implement. Health Aff (Millwood). 2015 Nov 1;34(11):1932-9.
- Institute of Medicine. Local Government Actions to Prevent Childhood Obesity, 2009. National Academies Press: Washington, DC.
Suggested Citation:Cradock AL, Gortmaker SL, Pipito A, Kenney EL, Giles CM. Washington: Sugar-Sweetened Beverage (SSB) Tax: Researching an Intervention to Create the Healthiest Next Generation [Issue Brief]. Washington State Department of Health, Olympia, WA, and the CHOICES Learning Collaborative Partnership at the Harvard T.H. Chan School of Public Health, Boston, MA; October 2017. |
The design for this brief and its graphics were developed by Molly Garrone, MA and partners at Burness.
This issue brief was developed at the Harvard T.H. Chan School of Public Health in collaboration with the Washington State Department of Health through participation in the Childhood Obesity Intervention Cost-Effectiveness Study (CHOICES) Learning Collaborative Partnership. This brief is intended for educational use only. Funded by The JPB Foundation. Results are those of the authors and not the funders. For more information, please visit: http://www.doh.wa.gov/CommunityandEnvironment/HealthiestNextGeneration/CHOICES


 Impact of Tax on Price to Consumers
Impact of Tax on Price to Consumers


 SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.5-7 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.8,9 The Dietary Guidelines for Americans, 201510 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.11-14 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.15
SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.5-7 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.8,9 The Dietary Guidelines for Americans, 201510 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.11-14 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.15
 SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.2-4 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.5-6 The Dietary Guidelines for Americans, 20157 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.8-11 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.12
SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.2-4 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.5-6 The Dietary Guidelines for Americans, 20157 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.8-11 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.12 Impact of Tax on Price to Consumers
Impact of Tax on Price to Consumers
 Background
Background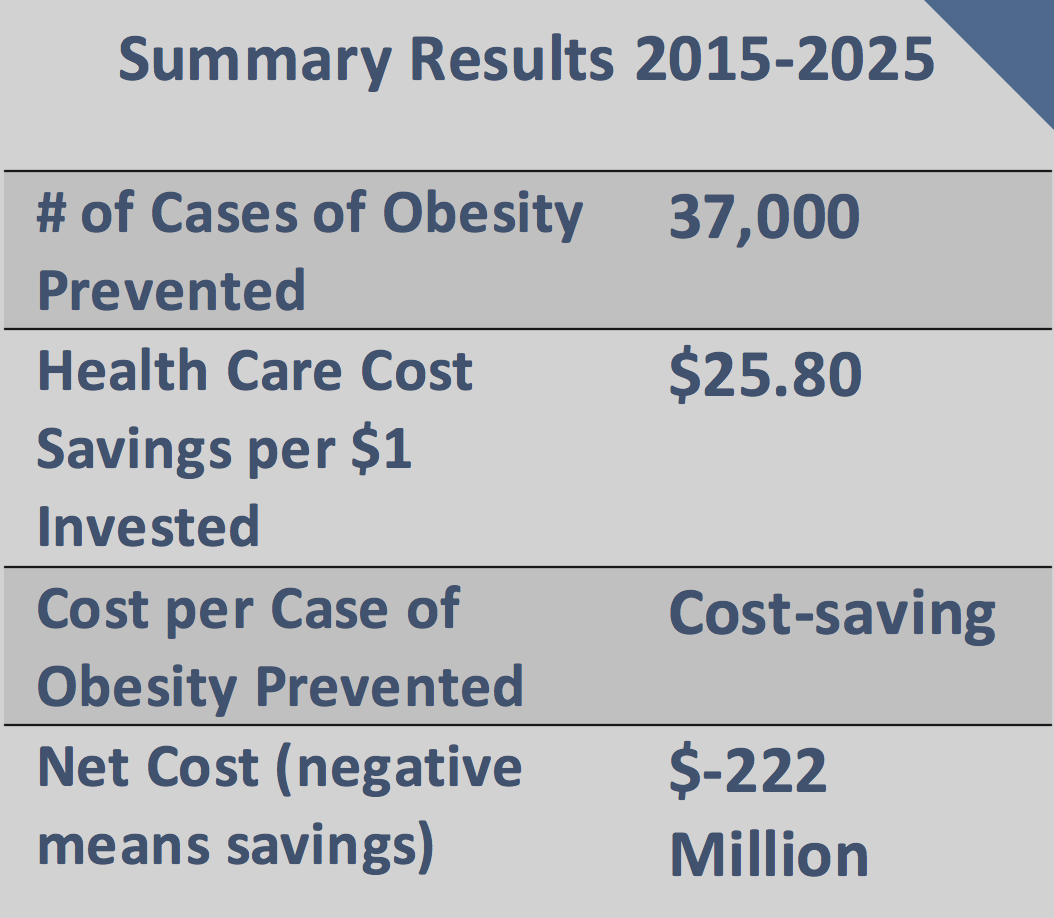

 SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.5-7 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.8,9 The Dietary Guidelines for Americans, 201510 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.11-14 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.15
SSBs include all beverages with added caloric sweeteners. The modeled excise tax does not apply to 100% juice, milk products, or artificially-sweetened beverages. Although SSB consumption has declined in recent years, children and adults in the U.S. consume twice as many calories from SSBs compared to 30 years ago.5-7 Randomized trials and longitudinal studies have linked SSB consumption to excess weight gain, diabetes, and cardiovascular disease. Consumption of SSBs increases the risk of chronic diseases through its impact on BMI and other mechanisms.8,9 The Dietary Guidelines for Americans, 201510 recommends that individuals reduce SSB intake in order to manage their body weight. Drawing on the success of tobacco taxation and decades of economic research, public health experts have called for higher taxes on SSBs and documented their likely impact.11-14 In 2009, the IOM recommended that local governments implement tax strategies to reduce consumption of “calorie-dense, nutrient-poor foods,” emphasizing SSBs as an apt target for taxation.15