
Dietz WH, Gortmaker SL. New Strategies to Prioritize Nutrition, Physical Activity, and Obesity Interventions. Am J Prev Med. 2016 Apr 26. pii: S0749-3797(16)30069-1.
Abstract
Interventions for obesity have not often been based on considerations that could predict their effectiveness. However, advances in research provide several new approaches that can inform priorities for public health interventions directed at nutrition, physical activity, and obesity. These approaches include estimation of the effect size, comparison of the calorie gap with the caloric deficit induced by the intervention, population reach and impact, cost and cost effectiveness of the intervention, time required to evaluate the effect of the intervention on weight change, and feasibility of the intervention. Incorporation of these considerations by policymakers and public health practitioners will help identify those interventions most likely to achieve changes in the prevalence of obesity.
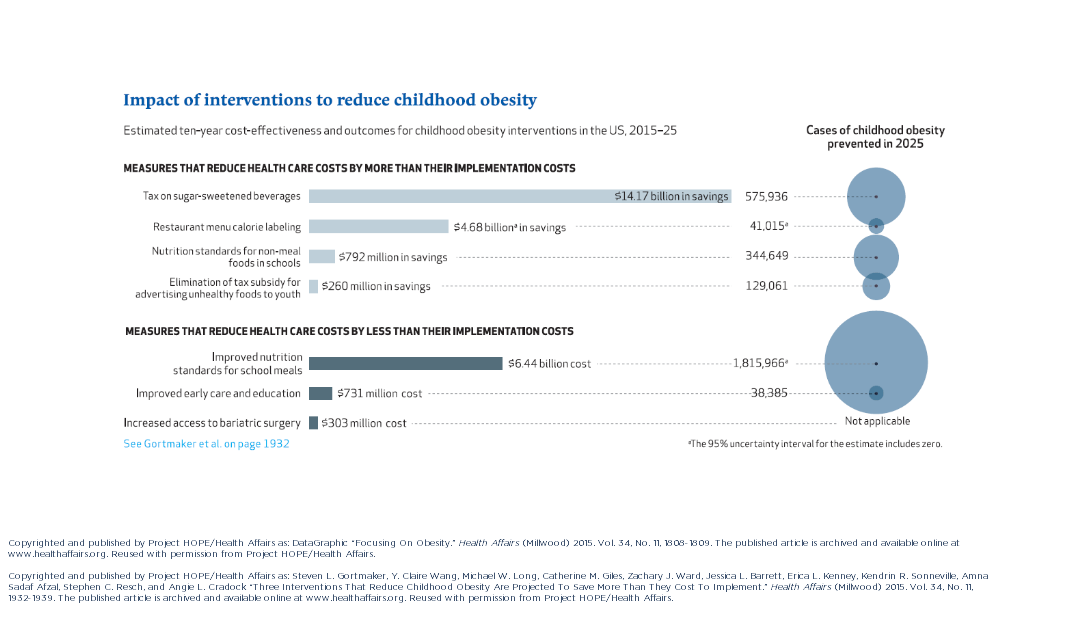


 “We know that the current level of sugar-sweetened beverage consumption in the United States is doing real harm to our children, our families, and our society by increasing the risk of obesity, diabetes, and cardiovascular disease, leading to increased healthcare costs and early deaths,” says lead study author
“We know that the current level of sugar-sweetened beverage consumption in the United States is doing real harm to our children, our families, and our society by increasing the risk of obesity, diabetes, and cardiovascular disease, leading to increased healthcare costs and early deaths,” says lead study author 
 “By changing the tax treatment of advertising expenses, the food industry will have less incentive to advertise unhealthy foods and drinks to kids,” says lead author Kendrin Sonneville, ScD, RD, Director of Nutrition Training in the Division of Adolescent Medicine at Boston Children’s Hospital.
“By changing the tax treatment of advertising expenses, the food industry will have less incentive to advertise unhealthy foods and drinks to kids,” says lead author Kendrin Sonneville, ScD, RD, Director of Nutrition Training in the Division of Adolescent Medicine at Boston Children’s Hospital.
 “Full day childcare programs are an educational environment responsible for providing children with snacks, meals, and daily opportunities for physical activity,” says lead author, Davene Wright, PhD, an Assistant Professor in the Department of Pediatrics at the University of Washington School of Medicine. “Many childcare programs fail to meet best practice standards for nutrition, physical activity, and screen time viewing. When 20 percent of preschool-aged children in the US are currently overweight or obese, this sector should be a key target for policy regulations to aid in the development of lifelong healthy behaviors.”
“Full day childcare programs are an educational environment responsible for providing children with snacks, meals, and daily opportunities for physical activity,” says lead author, Davene Wright, PhD, an Assistant Professor in the Department of Pediatrics at the University of Washington School of Medicine. “Many childcare programs fail to meet best practice standards for nutrition, physical activity, and screen time viewing. When 20 percent of preschool-aged children in the US are currently overweight or obese, this sector should be a key target for policy regulations to aid in the development of lifelong healthy behaviors.”
 Upon visiting an elementary school physical education (PE) class, you would expect to find children engaged in exercise. In reality, the typical PE class in the US may not be so active. While most elementary schools do require some PE, students on average spend less than half of class time engaged in moderate-to-vigorous physical activity (MVPA). Additionally, PE activity levels are lower when more class time is spent organizing students or reviewing rules and techniques, and when PE classes are led by classroom teachers instead of trained PE specialists.
Upon visiting an elementary school physical education (PE) class, you would expect to find children engaged in exercise. In reality, the typical PE class in the US may not be so active. While most elementary schools do require some PE, students on average spend less than half of class time engaged in moderate-to-vigorous physical activity (MVPA). Additionally, PE activity levels are lower when more class time is spent organizing students or reviewing rules and techniques, and when PE classes are led by classroom teachers instead of trained PE specialists.