A CHOICES study examined the impact of the Healthy, Hunger-Free Kids Act of 2010 on child obesity risk, and found that policies that strengthen nutritional standards for meals and beverages at schools may be effective tools for reducing obesity among children living in poverty.
Kenney EL, Barrett JL, Bleich SN, Ward ZJ, Cradock AL, Gortmaker SL. Impact Of The Healthy, Hunger-Free Kids Act On Obesity Trends. Health Aff. 2020;39(7). doi:10.1377/hlthaff.2020.00133

The study’s research team, led by Erica Kenney, examined the impact of the Healthy, Hunger-Free Kids Act of 2010 on child obesity risk. The legislation strengthened nutritional standards for meals and beverages provided through the National School Lunch, Breakfast, and Smart Snacks programs. The Act’s whole grain standards were relaxed under the Trump administration, but this change was struck down in federal court. Additional rollbacks of the Act’s standards have been proposed.
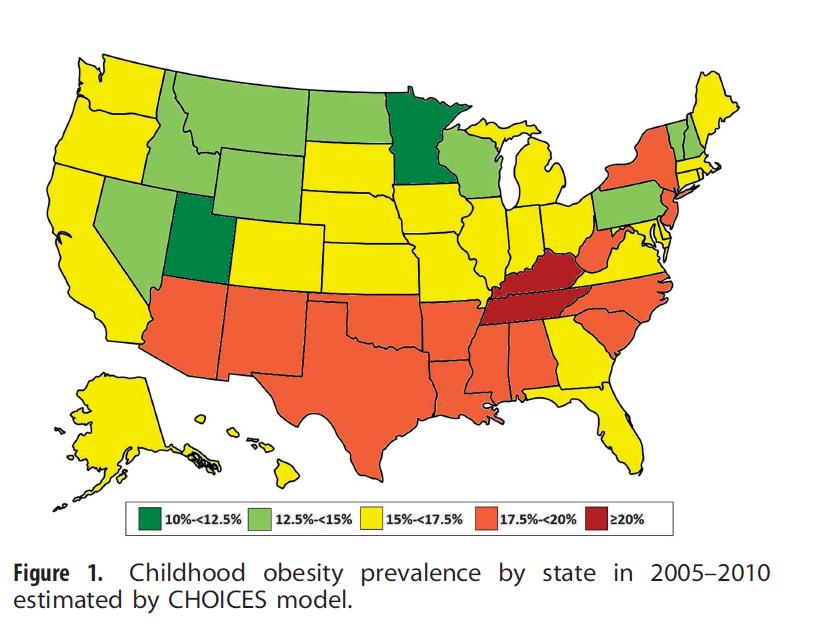
The researchers reviewed data for 173,013 youths taken from the National Survey of Children’s Health from 2003–2018, prior to when rollbacks went into effect.
While they found no significant association between the legislation and childhood obesity trends overall, they did find significant reductions in obesity risk among children living in poverty—a population that is particularly reliant on school meals. Among these children, the risk of obesity, which had been trending steadily upwards prior to the legislation going into effect, declined substantially each year following the act’s implementation, translating to a 47% reduction in obesity prevalence in 2018 from what would have been expected without the legislation.
The researchers conclude that the Healthy, Hunger-Free Kids Act’s science-based nutritional standards should be maintained to support healthy growth, especially among children living in poverty. They also suggest that policymakers consider strategies to increase participation in school meals programs.
“Based on our study, as well as research that USDA and other researchers have conducted showing improvements in diet, the improved school meals standards have been a great public health success story,” said first author Kenney. “These healthier school meals are helping to protect the health of the children who have been placed at highest risk for poor health, and they reduce hunger while also reducing their risk of chronic diseases later in life.”




 “It is clear that the most cost-effective strategies for preventing new cases of obesity are population-level approaches like taxes and school-based policies,” said
“It is clear that the most cost-effective strategies for preventing new cases of obesity are population-level approaches like taxes and school-based policies,” said 
 Though national guidelines from the U.S. Department of Health and Human Services (2008) recommend that both children and adolescents participate in 60 minutes or more of moderate to vigorous physical activity (MVPA) per day, many in this age group throughout the U.S. do not meet this standard. A variety of interventions can increase physical activity among youth, but implementation can be challenging for decision makers who have limited resources and implementation guidance.
Though national guidelines from the U.S. Department of Health and Human Services (2008) recommend that both children and adolescents participate in 60 minutes or more of moderate to vigorous physical activity (MVPA) per day, many in this age group throughout the U.S. do not meet this standard. A variety of interventions can increase physical activity among youth, but implementation can be challenging for decision makers who have limited resources and implementation guidance.